

Adults and children are both equally at risk to get their bones fractured from sports, accidents, falls and countless other misfortunes. Their bones, however, are quite different in a sense that, children’s bones are still growing, are soft and they have a layer within called a growth plate typically found at the ends of long bones. Growth plates function, as the name suggests, to increase the length of the bones as part of the child’s growth.
Children can get their growth plate fractured through one or the other mechanisms. Either they could get it from a singular event such as a fall or trauma from an accident, or through repetitive stress on the child’s bones that over time leads to fracture. Some factors may increase the likelihood of getting growth plate fracture. Among them are, gender; boys are more predisposed to get growth plate fractures because girls will stop growing earlier than boys. Next are those who engage in competitive sports like rugby, soccer, and also, recreational sports share the same risk, namely skateboarding, gymnastics and biking,
To understand growth plate fracture healing, we have to first understand the different types of growth plate fractures. This is important because different types of fracture signify the different degree of injury, hence affecting the outcome of healing. According to a widely used classification called the Salter-Harris Classification, there are 5 types of growth plate fractures.
Table of Contents
Type I Fracture
The fracture is within the growth plate and separates the bone end from the bone shaft.
Type II Fracture
The commonest type. The fracture breaks through a part of the growth plate and extends to the shaft.
Type III Fracture
The fracture breaks through the growth plate and extends to the bone end. This type of fracture is commonly seen in older children.
Type IV Fracture
The fracture extends through and through from the shaft, along with the growth plate and ends at the bone end.
Type V Fracture
A rare type. The fracture involves crushing injury to the growth plate from a compressive force.
Type I fracture carries the best prognosis, has the least complications, and outcome from treatment would leave little to no trace of impairments. Going down the list will carry with it poorer prognosis.
The approach to treat growth plate fractures varies according to a myriad of factors, such as which bone is involved, what type of fracture, how much and how severely the fragments of the bones are displaced, the age and health of the child and associated injuries along with the fracture.
Generally, the treatment modalities consist of surgical approach and a non-surgical approach.
Nonsurgical
Many growth plate fractures heal successfully with immobilization and that is our target of management. When we restrict the movement of the fractured limb, we are reducing the pain of the child, preventing further injuries at the site of the fracture, and we are promoting the ends of the broken bones to meet, heal and form a strong new connection.
We can achieve this through the use of casts. The limbs will be positioned in a specific manner to provide comfort and limit movements, and a cast will be applied to the injured limb. Sometimes, a sling may also be used to offer support.
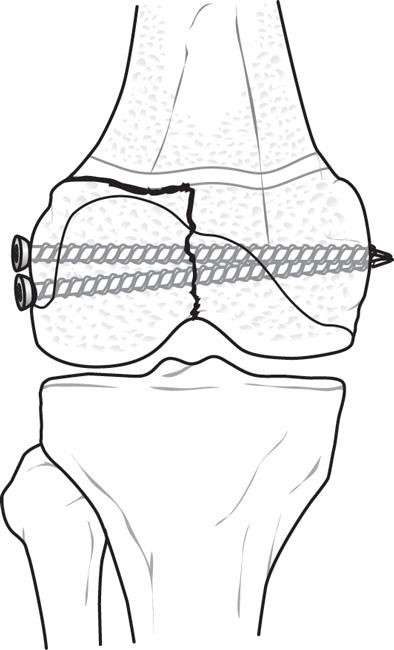
Surgical
In an unfortunate event wherein there are significant displacements, fragmentations, joint involvements, fractures that cannot be aligned, then surgery will be essential as part of the management. The most commonly done surgery involving growth plate fractures is open reduction and internal fixation. The bones will be manipulated as to achieve satisfactory alignment, this is called reduction, and the corrected bony parts will be fixed into place by means of screws, wires, or metal plates, and this part is called fixation.











